
Difference between labelled IOL power and actual power of the IOL
- Jul 3, 2024
- 6 min read
Updated: Jul 4, 2024
A common notion amongst clinicians is that the labelled power (diopter) on the IOL box is precisely the power of the IOL. That is, the labelled power of the IOL on the box corresponds to its exact focal length. This is not true. The International Organization for Standardization (ISO) as well as the American National Standards Institute (ANSI) provides some tolerances to the labelled IOL power on the box. These are(1):
For IOLs labelled between 0.0 D to 15.0 D, the labelled IOL power should be within +/- .30 D
For IOLs labelled between 15.0 D to 25.0 D, the labelled IOL power should be within +/- .40 D
For IOLs labelled between 25.0 D to 30.0 D, the labelled IOL power should be within +/- .50 D.
For IOLs labelled above 30.0 D, the labelled IOL power should be within +/- 1.0 D.
So if you are implanting a 12.0 diopter IOL, the actual power of the IOL could be anywhere between 11.70 D to 12.30 D. We know that achieving the refractive target is always difficult in short eyes. The labelled IOL power of 31.0 diopter could be anywhere between 30.0 to 32.0 diopter as per tolerances set by ISO and ANSI standards.
My own calculation of labelled IOL power of a commercially available 22.0 D lens with radius of curvature 1X.620* (anterior) and -2X.300* (posterior), with a lens thickness of .6X* mm, and a refractive index of (1.X4)*, showed the power of the IOL as per Gaussian thick lens formulae as 22.38 D. So much for the labelled IOL power on the IOL box, and its actual power when mathematically derived as per Gaussian thick lens formula with a aqueous and vitreous refractive index of 1.336 and 1.337, respectively (Fig 1)

The difference between the actual power and labelled IOL power may be due to a few reasons:
First, IOL power is available in .50 diopter of increments. So if the actual IOL power is 15.15 D, then it will be rounded off to a labelled IOL power as 15.0 D. On the other hand if the actual IOL power is 15.35 D, it would be labelled as 15.50 D. This makes sense, as the need of IOL power in .25 increments has been always debated and is not commercially available.
However, in this context, it may also make sense if the exact IOL power as measured by the IOL manufacturer is displayed in the IOL box along with its closest approximation to dioptric availability. This may help in IOL constant optimization or personalization, because the surgeon will know what was the absolute refractive error (in case of any) with the implanted IOL power with its true IOL power. For Aconstant personalization, the difference between the observed refractive error and true IOL power is more practical than the labelled IOL power.
For example, if 19,65 is the IOL power required for emmetropia, and the surgeon implants a rounded off labelled IOL power of 20.0 D ( providing a refraction of -.30) with exact IOL power labelled as 19.80 (providing a refraction of -.15) , landing the patient with +.50 diopter spherical, then the absolute and real error is .65 diopters ( -.15 plus +.50 diopter).
Without the exact IOL power spelled on the IOL box (that is with the current practice of approximated IOL power labelling), the absolute refractive error in this case is .80 diopters ( -.30 plus .50 diopter). While this may look like a small change, IOL constant optimization is a time consuming work, and we need to be as accurate as possible. Besides, the more the difference between the labelled IOL power and actual IOL power ( in higher power IOL beyond 25 diopters), more the need for such label for A constant personalization. Thus an IOL power labelled as 31.0 diopter may be anywhere between 30.0 diopter to 32.0 diopter. In extreme cases, where the labelled IOL power of 31.0 diopter is in reality 30.25 diopter, a large refractive surprise may be hard to avoid. In such cases, real IOL power labelling may be very helpful.
This brings us to the second reason, a question that involves the accuracy (or tolerance) to the labelled IOL power from its actual power.
Most IOL manufacturing companies would employ either of the following method to calculate the IOL focal length: image magnification, Talbot interferometry, Moire deflectometry, or confocal laser method (2). Regardless of the method used by the IOL manufacturer, inaccuracy in measurement can creep in from different areas. For example, the measurement itself may be limited by the limits of measurement of the device itself.
The ISO sets standards for measurement of IOL power(3). One of this is:
a) Determining the radius over a 3 mm diameter using a radius meter, interferometer, or optical coherence tomography, measuring the lens thickness with a micrometer. This is important to find out the principal planes of refraction, particularly the second principal plane. To understand the principal planes of refraction you can refer to my article Gaussian optics, Gullstrand eye, & Biometry by following the link https://www.quickguide.org/post/all-about-gaussian-optics-gullstrand-eye-theoretical-and-ray-tracing-formula or go through the video
b) Measuring back focal/effective focal length:
To obtain the back focal length (BFL), the distance from the back vertex of the IOL to the focal point is measured with a parallel light incident on-axis on the IOL.
The effective focal length (EFL) is the distance from the second principal plane to the focal point with parallel light incident on-axis on the IOL. The EFL can be measured with a nodal slide bench. These methods are better for conditions in the air and are suitable
for all IOLs.
Likewise standards are also set if IOL power is to be measured by image magnification method or by other methods.
In confocal laser method, that is often used by US FDA of late, as well as some IOL manufacturing companies, the IOL may be kept hydrated in room temperature of about 22 deg centigrade, and then mounted in a wet cell of about 35 deg centigrade. The back focal length is then measured at the paraxial region of the IOL, and adjusted with the manufacturer provided principal plane correction.
The third reason for IOL power discrepancy may be when there is a mismatch between temperature in which the optical power of the IOL is measured and our body temperature .
It is not usually spelled out by IOL manufacturers if the IOL power is measured in room temperature or a temperature that is closer to our body temperature. Standard testing environments should be used that mimics closely the body temperature. If the IOL is measured in room temperature, or if the IOL optical power is measured in a temperature condition that is lower than the body temperature, then as the IOL is implanted in the body, the dioptric power of the IOL will increase. This is usually taken into account for IOL power labelling by applying IOL power change to temperature changes. On an average IOL power was seen to increase by .13 diopters between the IOLs measured at 22 deg and 35 deg centigrade (2).
Another important parameter is the salinity of the liquid in which the IOL is measured to closely mimic the aqueous environment in which the IOL will finally seat in the patient's eye.If the refractive index of the saline solution is higher or lower than the true refractive index of aqueous, which is 1.336, then the optical power will vary.
The amount of aqueous absorption of the IOL material once implanted in the eye, will also change the refractive index of the IOL as well as the radius of curvature of the IOL, both of which will impact the final optical power of the IOL.
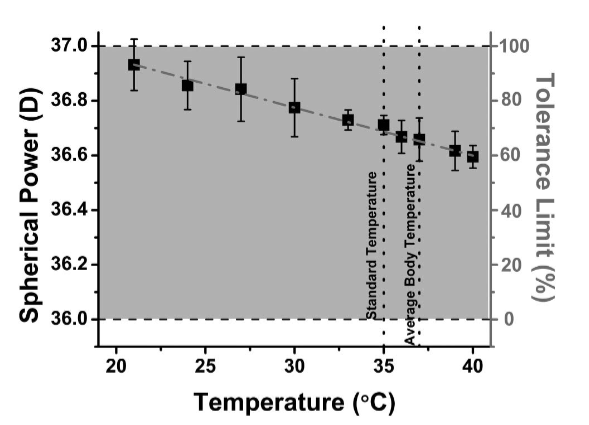
Benett Walker and co-authors studied the impact of temperature changes on the optical power of the IOL (4). They observed change in optical power of the lens as the temperature was increased from 20 deg C to 40 deg C. In the below image sourced from the study (4) you can observe the variation of spherical power at different temperatures. These variations are within the tolerance limit set forth by the ISO, but if IOLs are measured in room temperature then the variation of IOL power will be large at body temperature. The authors also noted the change in spherical aberration and cylinder components of the IOL through variation of temperature.
In this short article, I have tried to break some common notion about the labelled IOL power. I believe it is important that true or real IOL power should also be mentioned in the IOL box along with the existing practice of IOL power labelling that is close to IOL diopter availability in .50 D increments. IOL manufacturers should also spell out the standard IOL optical property testing protocol followed for IOL power labelling that will help in standardization of IOL power labelling for more precise refractive outcomes.
*Information hidden so as not to disclose brands.

References:
International Organization for Standardization. Ophthalmic im-plants – Intraocular lenses – Part 2: Optical Properties and Test Methods. Geneva, Switzerland, ISO, 1999 (ISO 11979-2
Testing the dioptric power accuracy of exact-power-labeled intraocular lenses November 2009Journal of Cataract and Refractive Surgery 35(11):1995-9
Mari Carmen García-Domene a, b, *, María Amparo Díez-Ajenjo a, b, Cristina Peris-Martínez a, Amparo Navea a, Jose María Artigas, A rapid method for measuring intraocular lens power in vitro with focimeter; https://doi.org/10.1016/j.exer.2015.09.009
Bennett N. Walker,1,* Robert H. James,1 Don Calogero,2 and Ilko K. Ilev1 - Impact of environmental temperature on opticalpower properties of intraocular lenses; 20 January 2014 / Vol. 53, No. 3 / APPLIED OPTICS


