
Complete Guide to IOL Power Calculation - Advanced Masterclass
- Feb 23
- 20 min read
The topics discussed in Masterclass are at an advanced level!
If you have not covered the basics, you are requested to first go through the Biometry section in this website, before you take the course.
The Masterclass in biometry is constantly updated.
Section 1
Understanding Modern IOL power calculation formula architecture:1.1 Why different IOL power calculation formula behave differently
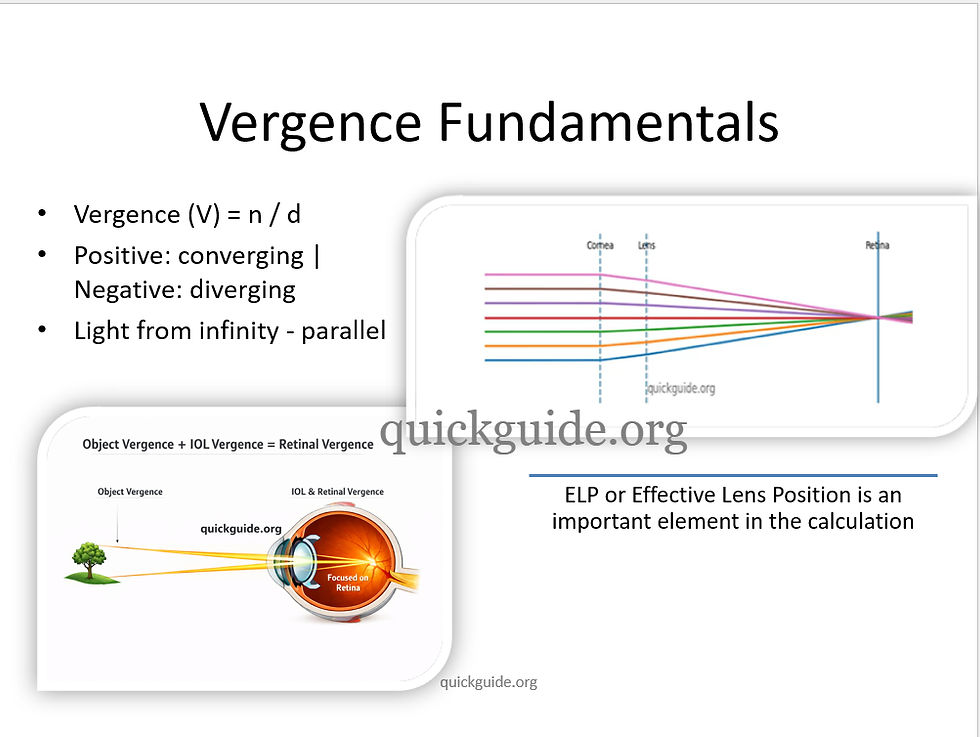
Vergence describes how “converging” or “diverging” a bundle of light rays is at a given plane in the eye. Parallel rays of light has zero vergence. As light rays pass through the cornea, the optical power of cornea makes the light rays converge. Vergence describes the converging power of cornea and how far the rays of light will travel further to reach the lens. Thus vergence studies the power of the cornea and the lens to converge the rays of light and the distance the rays of light travel, after passing through bother cornea and lens to reach the retina.
Vergence formula, v = n/d where n is the refractive index of medium and d is the distance the rays of light travel.
Thus all modern IOL formulas are fundamentally vergence based formula. First, they study the vergence of light rays (L) at the IOL plane, the emergent vergence of light rays (L') after they emerge passing through the IOL (which will have a certain power F).
The formula is therefore,

In the equation above, vergence of light rays after passing through the IOL will have to take into account the refractive index of vitreous (numerator). The denominator, AL-ELP signifies the posterior segment length up to the retina (ELP is the distance between the cornea and the refracting plane of the IOL)
Similarly, the vergence of incoming rays of light that pass through the cornea and reach the IOL has to be also taken into account.

By adding the vergence of equation in Fig 2a and 2b, we can arrive at the power of IOL. Remember, the above explanation is applicable to vergence based on thin optics lens provided by the mathematician, Gauss.
Next we will see IOL calculation formula according to thin and thick lens mathematical formulas.
1.2
How do thin and thick lens IOL calculation vergence-based formulas differ?
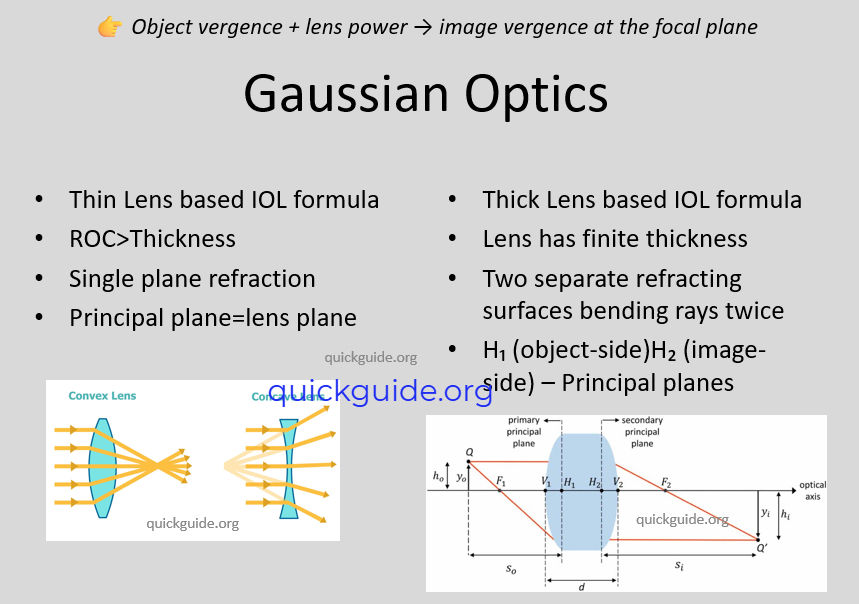
Power of any lens, be it glass power, or a lens used in microscope or telescope can be calculated mathematically by Gauss thin and/or thick lens formula. In a thin lens formula, provided by Gauss, the lens is considered to be so thin that the thickness of the lens is not considered. The entire refraction is considered to happen in only one plane. IOL calculation formulas of second and third generation, like the SRK T, Hoffer Q, the Holladay I, etc. are based on thin lens optical formula of Gauss. ELP or effective lens position is the distance from the cornea to the refraction plane of the IOL.
In this context, it is important to remember that the ELP is not a physical distance from the cornea to the IOL refraction plane. It is a virtual value that is back-calculated from post operative refraction of pseudophakic patients, and built in the formula. It is a virtual distance, and not a physical distance from the cornea to the IOL refraction plane.

On the other hand in thick lens formula, the lens thickness is taken into account. Thus in
thick lens formula there are two planes of refraction. These are the first and second
principal planes. For a biconvex IOL, the two principal planes sit inside the IOL. The focal
length of the IOL is the distance from the second principal plane to the point where all
rays of light converge.

1.3
Which IOL formulas utilize the vergence formula for thin and thick optics?
The below (Fig 6) describes IOL power calculation formula that are based on vergence based thin optics or thick optics formula.

The older two variable formula like the SRK T, Hoffer Q and Holladay I are based on thin optics vergence formula. These formulas do not consider the IOL as a thick optics lens. They assume that the entire refraction is happening in one single plane in the IOL.



